Scientists at the Johns Hopkins Kimmel Cancer Center have identified 16 genes that breast cancer cells use to survive in the bloodstream after they’ve escaped the low-oxygen regions of a tumor. Each is a potential therapeutic target to stop cancer recurrence, and one – MUC1 – is already in clinical trials.
The research was published online September 28 in the journal Nature Communications.
Deep in a tumor, full of rapidly dividing cells, cancer cells are faced with a lack of oxygen, a condition called hypoxia. Cancer cells that survive these tough environments end up seeking what they missed, slowly making their way to the oxygen-rich bloodstream and often seeding metastasis elsewhere in the body, explains lead study author Daniele Gilkes, Ph.D., an assistant professor of oncology at Johns Hopkins.
The team identified 16 genes responsible for this protection from reactive oxygen species, “which is a stress that occurs when the cells enter the bloodstream,” Gilkes says. “Although the hypoxic cells are localized in what we call the perinecrotic region of a tumor — meaning they’re sitting right next to dead cells — we think that they’re able to migrate into higher [oxygen] levels where they can actually find the bloodstream,” she says. “Cells able to survive super-low oxygen concentrations do a better job of surviving in the bloodstream. This is how, even after a tumor is removed, we sometimes find that cancer cells have set up elsewhere in the body. Lower levels of oxygen in a tumor correlate with worse prognosis.”
The scientists sought to learn what helps these post-hypoxic cells survive in an environment that would kill other cancer cells, and which genes were being turned on to facilitate survival.
In laboratory studies, Gilkes’ team color-coded hypoxic cells green, then applied a technique called spatial transcriptomics to identify which genes were turned on in the perinecrotic region, and that stayed on when the cells migrated to more oxygenated tumor regions. They compared cells in the primary tumors of mice with those that had entered the blood stream or the lungs. A subset of hypoxia-induced genes continued to be expressed long after cancer cells escaped the initial tumor.
“The results suggest the potential for a sort of memory of exposure to hypoxic conditions,” says Gilkes.
The new research showed a disparity between what occurs in laboratory models and what happens in the human body, solving a mystery that was puzzling scientists. When cells in a dish are hypoxic and returned to high levels of oxygen in a short time, they tend to stop expressing the (hypoxia-induced) genes and go back to normal. However, in tumors, hypoxia can be more of a chronic condition, not acute. When Gilkes’ team exposed cells to hypoxia for a longer period — five days was usually enough — they mimicked what was happening in the mouse models.
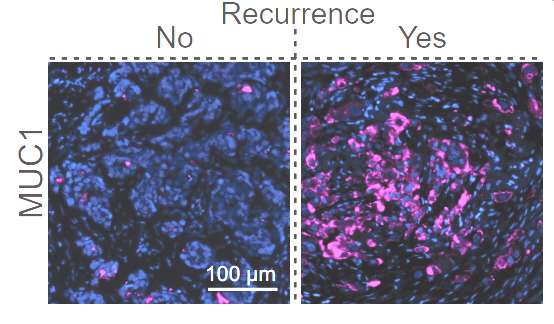
Results were particularly predictive for triple-negative breast cancer (TNBC), which has a high rate of recurrence. The researchers found that patient biopsies from TNBC that had recurred within three years had higher levels of a protein called MUC1.
As part of their research model, Gilkes and team blocked MUC1 using a compound called GO-203 to see if it would reduce the spread of breast cancer cells to the lung. Their aim was to specifically eliminate aggressive, post-hypoxic metastatic cells.
“If we reduced the level of MUC1 in these hypoxic cells, they were no longer able to survive in the bloodstream or in presence of reactive oxygen species, and they formed fewer metastases in mice,” Gilkes says. However, there are other factors at play, she says, and additional research will be needed to see if this finding is true across cancer types.
A phase I/II clinical trial targeting MUC1 for patients with advanced cancers across a variety of solid tumor types — including those found in breast, ovarian, and colorectal cancer — is ongoing, Gilkes says.
Study co-authors were Inês Godet, Harsh Oza, Yi Shi, Natalie Joe, Alyssa Weinstein, Jeanette Johnson, Michael Considine, Swathi Talluri, Jingyuan Zhang, Reid Xu, Steven Doctorman, Genevieve Stein-O’Brien, Luciane Kagohara, Cesar Santa-Maria and Elana Fertig, from Johns Hopkins, and Delma Mbulaiteye from the NIDDK STEP-UP Program at the National Institutes of Health.
The work was funded by The Jayne Koskinas Ted Giovanis Foundation for Health and Policy, the NCI/ SKCCC Core grant number P50CA006973, NCI grant number 5U01CA253403-03, and the National Cancer Center.
Santa-Maria has received research funds from AstraZeneca, GSK/ Tesaro, Merck, Gilead, Celldex, BMS and Pfizer, and consulting fees from Seattle Genetics. Fertig serves on the scientific advisory board of Resistance Bio, is a consultant for Merck and Mestag Therapeutics, and has received research funding from Abbvie, Inc. and Roche/Genentech. These relationships are managed by The Johns Hopkins University in accordance with its conflict-of-interest policies.
